
 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Cardiac Cycle - Isovolumetric Contraction (Phase 2)
All Valves Closed
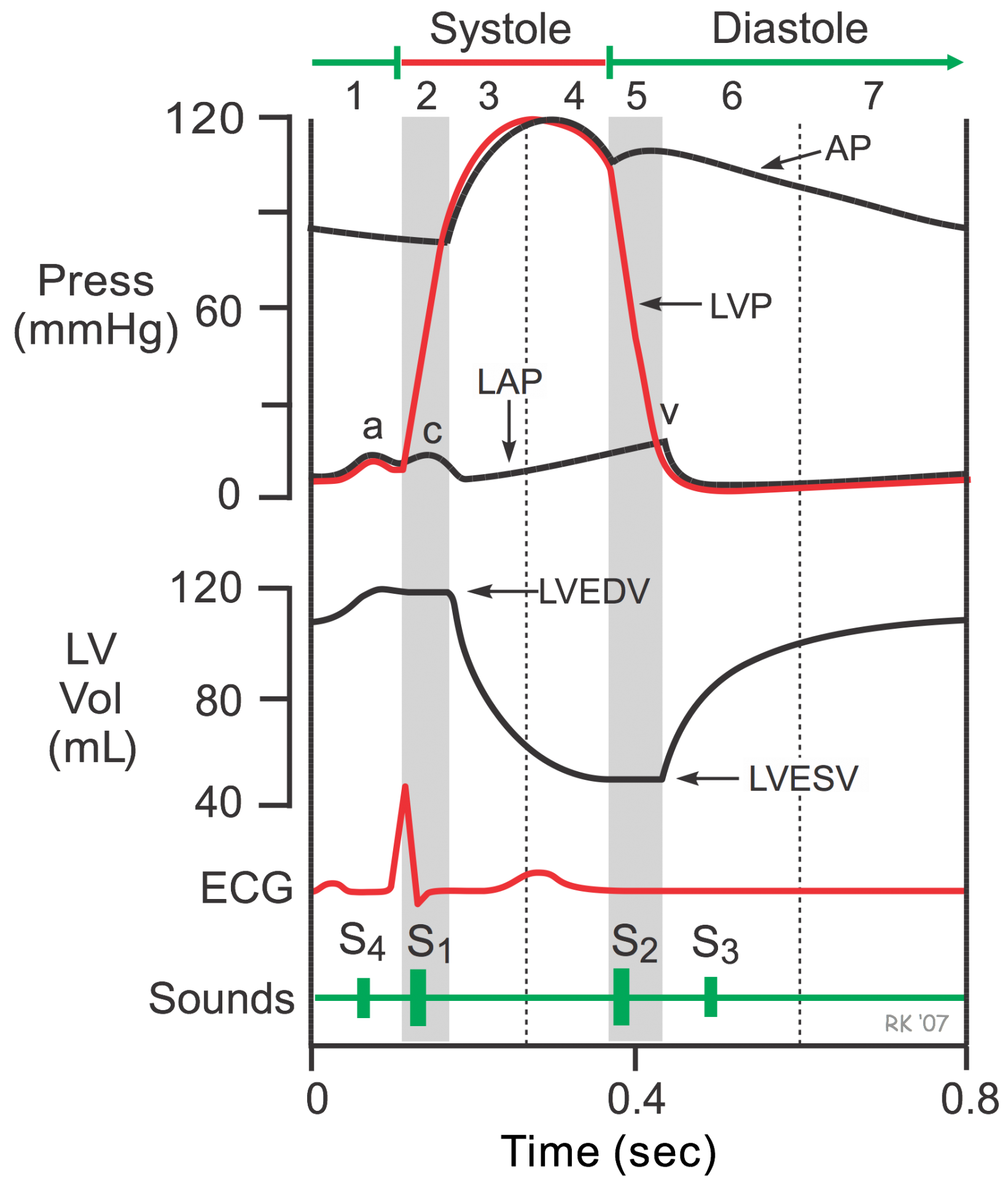 The second phase of the cardiac cycle (isovolumetric contraction) begins with the appearance of the QRS complex of the ECG, which represents ventricular depolarization. This triggers excitation-contraction coupling, myocyte contraction and a rapid increase in intraventricular pressure. Early in this phase, the rate of pressure development becomes maximal. This is referred to as maximal dP/dt.
The second phase of the cardiac cycle (isovolumetric contraction) begins with the appearance of the QRS complex of the ECG, which represents ventricular depolarization. This triggers excitation-contraction coupling, myocyte contraction and a rapid increase in intraventricular pressure. Early in this phase, the rate of pressure development becomes maximal. This is referred to as maximal dP/dt.
The AV valves close when intraventricular pressure exceeds atrial pressure. Ventricular contraction also triggers contraction of the papillary muscles with their chordae tendineae that are attached to the valve leaflets. This tension on the AV valve leaflets prevents them from bulging back into the atria and becoming incompetent (i.e., “leaky”). Closure of the AV valves results in the first heart sound (S1). This sound is normally split (~0.04 sec) because mitral valve closure precedes tricuspid closure.
During the time between the closure of the AV valves and the opening of the aortic and pulmonic valves, ventricular pressure rises rapidly without a change in ventricular volume (i.e., no ejection occurs). Ventricular volume does not change because all valves are closed during this phase. Contraction, therefore, is "isovolumic" or "isovolumetric." Individual myocyte contraction, however, is not necessarily isometric because individual myocytes undergo length changes. Some individual fibers contract isotonically (i.e., concentric, shortening contraction), whereas other fibers contract isometrically (i.e., no length change) or eccentrically (i.e., lengthening contraction). Therefore, ventricular chamber geometry changes considerably as the heart becomes more spheroid in shape. The chamber circumference increases and the atrial base-to-apex length decreases.
The rate of pressure increase in the ventricles is determined by the rate of contraction of the muscle fibers, which is determined by mechanisms governing excitation-contraction coupling. The maximal rate of pressure change during this phase is termed "dP/dtmax."
The c-wave noted in the LAP may be caused by bulging of mitral valve leaflets back into the left atrium. Just after the peak of the c wave is the x'-descent.
Jump to other phases:
- Phase 1 - Atrial Contraction
- Phase 3 - Rapid Ejection
- Phase 4 - Reduced Ejection
- Phase 5 - Isovolumetric Relaxation
- Phase 6 - Rapid Filling
- Phase 7 - Reduced Filling
Revised 11/04/2023