
 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Systolic and Diastolic Murmurs
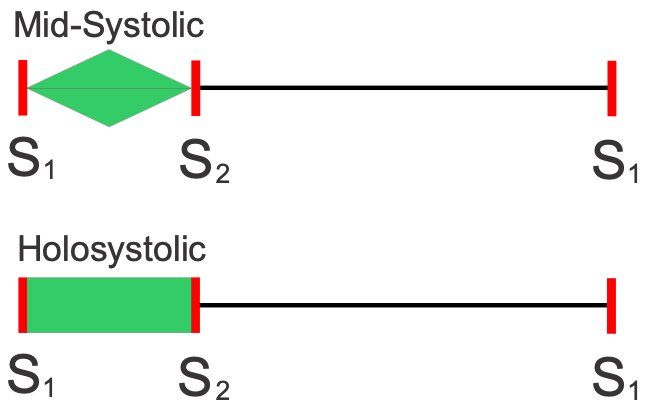 Systolic murmurs occur between S1 and S2 (first and second heart sounds), and therefore are associated with mechanical systolic and ventricular ejection. Mid-systolic murmurs typically have a crescendo-decrescendo character; they start softly and become loudest near mid-systole, followed by a decrease in sound intensity (see figure). This type of murmur is caused by either aortic or pulmonic valve stenosis. A second type of systolic murmur is holosystolic (sometimes called pansystolic) because the intensity is high throughout systole, as shown in the figure. This type of murmur is caused by mitral or tricuspid valve regurgitation, or by a ventricular septal defect.
Systolic murmurs occur between S1 and S2 (first and second heart sounds), and therefore are associated with mechanical systolic and ventricular ejection. Mid-systolic murmurs typically have a crescendo-decrescendo character; they start softly and become loudest near mid-systole, followed by a decrease in sound intensity (see figure). This type of murmur is caused by either aortic or pulmonic valve stenosis. A second type of systolic murmur is holosystolic (sometimes called pansystolic) because the intensity is high throughout systole, as shown in the figure. This type of murmur is caused by mitral or tricuspid valve regurgitation, or by a ventricular septal defect.
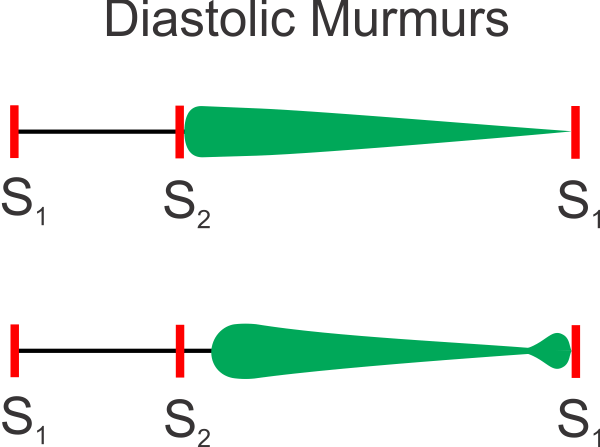 Diastolic murmurs occur after S2 and before S1; they are therefore associated with ventricular relaxation and filling. Such murmurs may be caused by aortic or pulmonic valve regurgitation. With outflow tract insufficiency (e.g., aortic valve), regurgitation begins immediately after S2 and quickly reaches maximal intensity, which then diminishes throughout diastole (decrescendo murmur) as shown in the top portion of the figure. A diastolic murmur may also be caused by mitral or tricuspid valve stenosis. With atrioventricular valve stenosis (e.g., mitral valve), the murmur is delayed beyond S2 when the ventricular pressure falls below atrial pressure and the atrioventricular valve opens. The sound is most intense early in diastole, then declines in intensity (decrescendo murmur). Near the end of diastole, atrial contraction can cause a brief increase in murmur intensity, as shown in the bottom portion of the figure.
Diastolic murmurs occur after S2 and before S1; they are therefore associated with ventricular relaxation and filling. Such murmurs may be caused by aortic or pulmonic valve regurgitation. With outflow tract insufficiency (e.g., aortic valve), regurgitation begins immediately after S2 and quickly reaches maximal intensity, which then diminishes throughout diastole (decrescendo murmur) as shown in the top portion of the figure. A diastolic murmur may also be caused by mitral or tricuspid valve stenosis. With atrioventricular valve stenosis (e.g., mitral valve), the murmur is delayed beyond S2 when the ventricular pressure falls below atrial pressure and the atrioventricular valve opens. The sound is most intense early in diastole, then declines in intensity (decrescendo murmur). Near the end of diastole, atrial contraction can cause a brief increase in murmur intensity, as shown in the bottom portion of the figure.
Revised 11/05/2023