
 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Ankle-Brachial Pressure Index
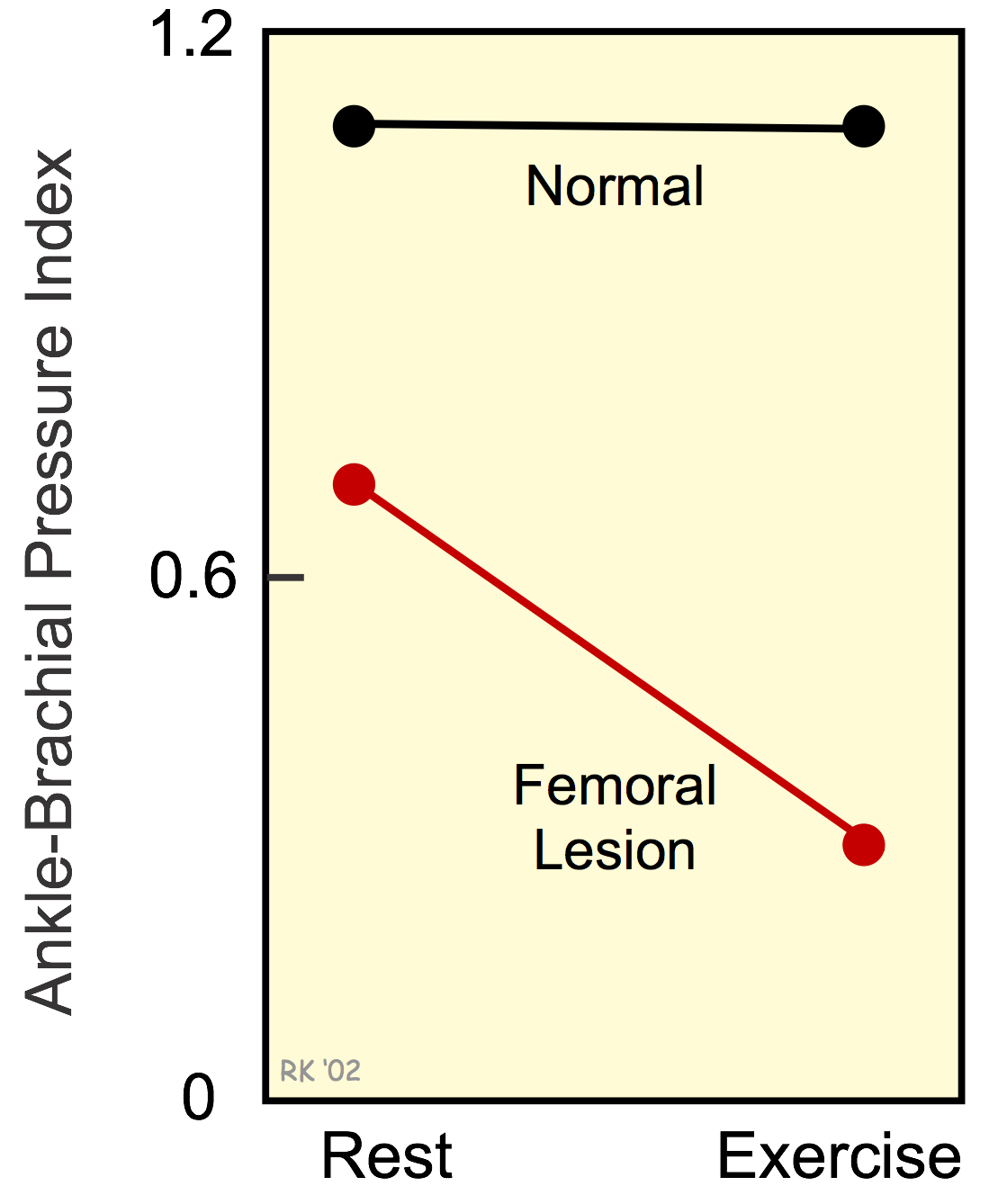 When stenotic lesions are present in major arteries of the leg (except the deep femoral and internal iliac arteries), the systolic pressure measured at the ankle will be reduced relative to the systolic pressure measured in the brachial artery of the arm. The ratio of ankle systolic pressure to brachial artery systolic pressure is termed the ankle-brachial pressure index (ABI) and is normally about 1.1. The normal ratio exceeds 1.0 because the shape of the arterial pressure pulse changes as it travels from the ascending aorta to the periphery, with the systolic pressure normally increasing and the diastolic pressure falling at peripheral sites. An ABI of <0.9 indicates arterial stenosis within the limb, located upstream (proximal) to the ankle. In the figure, the resting ABI of 0.7 indicates a moderate proximal occlusion. Severe stenosis is associated with resting leg pain and an ABI <0.5. An abnormally elevated ABI (>1.3) suggests "stiff" arterial vessels that may be found in diabetic and elderly patients.
When stenotic lesions are present in major arteries of the leg (except the deep femoral and internal iliac arteries), the systolic pressure measured at the ankle will be reduced relative to the systolic pressure measured in the brachial artery of the arm. The ratio of ankle systolic pressure to brachial artery systolic pressure is termed the ankle-brachial pressure index (ABI) and is normally about 1.1. The normal ratio exceeds 1.0 because the shape of the arterial pressure pulse changes as it travels from the ascending aorta to the periphery, with the systolic pressure normally increasing and the diastolic pressure falling at peripheral sites. An ABI of <0.9 indicates arterial stenosis within the limb, located upstream (proximal) to the ankle. In the figure, the resting ABI of 0.7 indicates a moderate proximal occlusion. Severe stenosis is associated with resting leg pain and an ABI <0.5. An abnormally elevated ABI (>1.3) suggests "stiff" arterial vessels that may be found in diabetic and elderly patients.
Patients with occlusive arterial disease in the leg typically experience claudication (leg pain when walking). As a person walks, increased oxygen demand in the lower limb increases its need for oxygen, and therefore, flow increases across the proximal stenotic lesion, which supplies flow to the lower limb. This increases the pressure drop across the occlusive lesion, causing distal pressures to fall. In summary, as shown in the figure, the ABI decreases during exercise when there is a proximal stenotic lesion. When the proximal arteries are normal, there is only a small decline in the ABI during leg exercise.
An excellent video resource from Stanford School of Medicine showing how ABI is measured in a patient is shown below.
Revised 01/30/2023