
 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Ventricular Compliance
 As the ventricle fills with blood, the pressure and volume that result from filling are determined by the compliance of the ventricle. Normally, compliance curves are plotted as the change in volume (ΔV) over the change in pressure (ΔP). For the ventricle, however, it is common to plot ΔP versus ΔV (see Figure). Therefore, the slope of the relationship is the reciprocal of the compliance, which is sometimes referred to as ventricular "stiffness."
As the ventricle fills with blood, the pressure and volume that result from filling are determined by the compliance of the ventricle. Normally, compliance curves are plotted as the change in volume (ΔV) over the change in pressure (ΔP). For the ventricle, however, it is common to plot ΔP versus ΔV (see Figure). Therefore, the slope of the relationship is the reciprocal of the compliance, which is sometimes referred to as ventricular "stiffness."
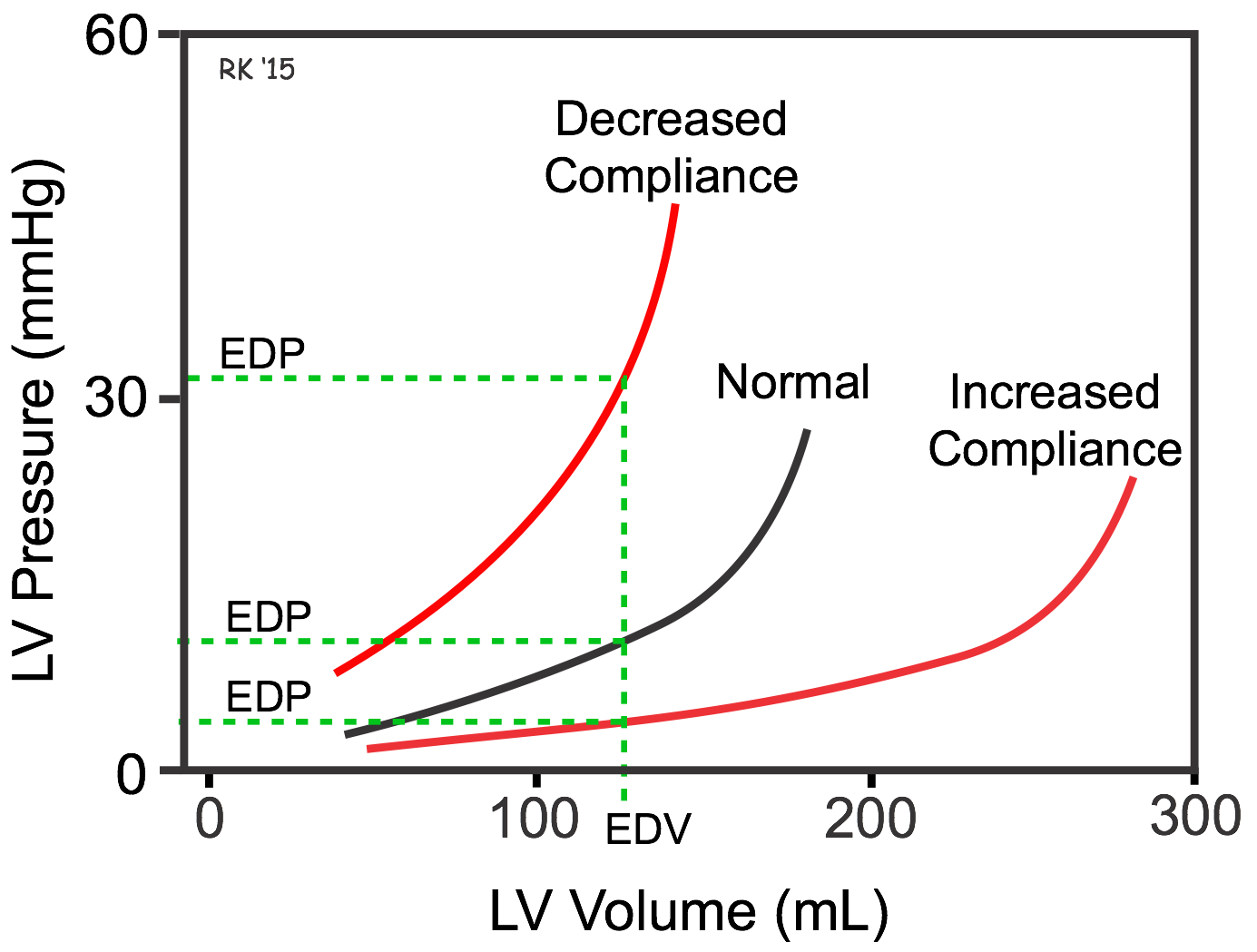
As the ventricle fills with blood and its volume increases, the pressure within the ventricular chamber passively increases (see the Normal filling curve in the figure). The relationship is not linear, particularly at higher volumes because the compliance of the ventricular wall decreases ("stiffness" increases) the more the ventricular wall is stretched. This occurs in most biological tissues.
The compliance of the ventricle is determined by the structural properties of the cardiac muscle (e.g., muscle fibers and their orientation, and connective tissue) as well as by the state of ventricular contraction and relaxation. For example, in ventricular hypertrophy the ventricular compliance is decreased (i.e., the ventricle is "stiffer") because the thickness of the ventricular wall increases; therefore, ventricular end-diastolic pressure (EDP) is higher at any specific end-diastolic volume (EDV) (see Figure). Alternatively, at a given EDP, a less compliant ventricle would have a smaller EDV (i.e., filling will be impaired). Other cardiac disease states, such as restrictive cardiomyopathy, can also decrease in ventricular compliance. If ventricular relaxation is impaired (as occurs in some forms of diastolic heart failure), the functional ventricular compliance is reduced, which will impair ventricular filling. In a disease state, such as dilated cardiomyopathy, the ventricle remodels and becomes very dilated without appreciable thickening of the wall. This dilated ventricle will have increased compliance, as shown in the figure; therefore, although the EDV may be very high, the EDP may not be elevated appreciably.
A 10-minute lecture on this topic can be viewed by clicking on Ventricular Compliance.
Revised 01/24/2023