
 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Stress Relaxation
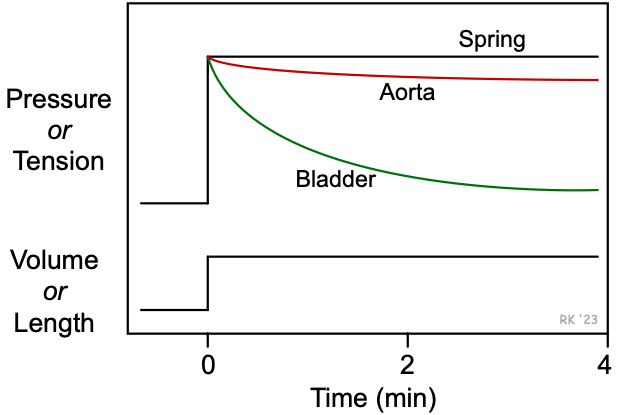 Stress relaxation is a property of biological tissues that is related to their viscoelastic properties. To understand this concept, the stress-strain relationships for a spring and biological tissues such as a blood vessel and bladder can be compared (see figure). When a spring is suddenly stretched (increased strain applied), the tension (stress) that is generated is proportional to the change in length (i.e., Hookean behavior). Furthermore, the developed tension remains constant. In contrast, if a blood vessel (e.g., aortic segment) is isolated, tied off at one end and cannulated at the other end so that it can be filled with a known volume of fluid and have its pressure measured simultaneously, then a sudden increase in volume (strain) increases pressure (stress); however, the pressure does not remain steady, but declines a small amount over time. This decline in pressure (stress) over time at a constant volume (strain) is termed "stress relaxation." The reason that pressure falls while the volume remains constant can be explained by the Law of LaPlace, where wall tension (T) is proportional to pressure (P) times radius (r), T ∝ P⋅r. When this expression is rearranged and solved for pressure, then P ∝ T/r. Therefore, pressure can fall at a constant radius (or volume) if wall tension decreases over time, and this occurs during stress relaxation. If an analogous experiment was performed on the bladder, the stress relaxation would be much greater and occur more rapidly.
Stress relaxation is a property of biological tissues that is related to their viscoelastic properties. To understand this concept, the stress-strain relationships for a spring and biological tissues such as a blood vessel and bladder can be compared (see figure). When a spring is suddenly stretched (increased strain applied), the tension (stress) that is generated is proportional to the change in length (i.e., Hookean behavior). Furthermore, the developed tension remains constant. In contrast, if a blood vessel (e.g., aortic segment) is isolated, tied off at one end and cannulated at the other end so that it can be filled with a known volume of fluid and have its pressure measured simultaneously, then a sudden increase in volume (strain) increases pressure (stress); however, the pressure does not remain steady, but declines a small amount over time. This decline in pressure (stress) over time at a constant volume (strain) is termed "stress relaxation." The reason that pressure falls while the volume remains constant can be explained by the Law of LaPlace, where wall tension (T) is proportional to pressure (P) times radius (r), T ∝ P⋅r. When this expression is rearranged and solved for pressure, then P ∝ T/r. Therefore, pressure can fall at a constant radius (or volume) if wall tension decreases over time, and this occurs during stress relaxation. If an analogous experiment was performed on the bladder, the stress relaxation would be much greater and occur more rapidly.
Therefore, different biological tissues display different degrees of stress relaxation. The reason for these differences among tissues is that tissues differ in their structural components (e.g., smooth muscle, collagen, elastin) and the arrangement of those components within the tissue. For example, the bladder, which is mostly smooth muscle, shows a high degree of stress relaxation, whereas a tendon that is primarily composed of collagen shows virtually no stress relaxation.
To understand the functional significance of stress relaxation, one only has to relate the ability of different tissues to display stress relaxation to their biological function. For example, as urine flows into the bladder, the bladder volume increases. It is important that as the volume increases, there is only a small increase in pressure, otherwise high pressures within the bladder would impede urine outflow from the kidneys and damage the kidneys. The high compliance and high degree of stress relaxation in the bladder ensures that the pressure does not increase much. If the aorta and other arterial vessels showed the same high magnitude of stress relaxation as the bladder, then blood pressure could not be sufficiently maintained.
Understanding stress relaxation is important when the compliance of a tissue is being determined. Compliance is the ratio of the change in volume divided by the change in pressure. However, because tissues such as blood vessels show some level of stress relaxation, it is important to measure the steady-state change in pressure after the volume is increased. If the pressure is measured before stress relaxation is complete, then the measured compliance would be lower than that measured in the steady-state. If the volume changes rapidly within a blood vessel (e.g., the aorta during cardiac systole and diastole), the measured compliance (change in volume divided by the change in pressure) will vary depending upon the rate of volume change. With more rapid changes in volume (e.g., as occurs with increased ventricular ejection velocity), the calculated compliance will be less than at more slowly changing volumes. Therefore, when a true steady-state compliance cannot be determined, the compliance is sometimes referred to as the "dynamic compliance" of the tissue or organ.
Revised 12/8/2022