
 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Arachidonic Acid Metabolites (Prostaglandins and Related Compounds)
Prostaglandins and related compounds (collectively referred to as prostanoids or eicosanoids) such as prostacyclin (PGI2), leukotrienes (LTs) and thromboxanes (TXs) are produced by many cells in the body. Although their primary physiological actions are related to inflammation and hemostasis, by nature they all are vasoactive and can modulate cardiovascular function, particularly vascular tone. Their effects are very localized because they are paracrine hormones that are released by one cell and act on nearby cells.
Prostanoids
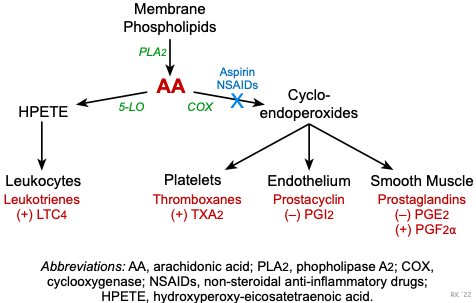 Prostanoids are fatty acid compounds derived from membrane phospholipids. When these phospholipids are acted upon by phospholipase A2, arachidonic acid is formed. Two important pathways for arachidonic acid metabolism are the cyclooxygenase (COX) and 5-lipoxygenase (5-LO) pathways. The COX pathway forms intermediate compounds called cyclo-endoperoxides (PGG2 and PGH2). Enzymes, many of which are tissue-specific, then convert the cyclo-endoperoxides into the final biologically active prostanoid.
Prostanoids are fatty acid compounds derived from membrane phospholipids. When these phospholipids are acted upon by phospholipase A2, arachidonic acid is formed. Two important pathways for arachidonic acid metabolism are the cyclooxygenase (COX) and 5-lipoxygenase (5-LO) pathways. The COX pathway forms intermediate compounds called cyclo-endoperoxides (PGG2 and PGH2). Enzymes, many of which are tissue-specific, then convert the cyclo-endoperoxides into the final biologically active prostanoid.
There are different forms of COX, two of which are COX-1 and COX-2. Aspirin and other non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and acetaminophen (Tylenol®) are non-selective inhibitors of the COX enzymes. Newer NSAIDs are relatively selective for COX-2, and have fewer gastrointestinal-related side effects. COX-1 is constitutive and therefore produces prostanoids under basal conditions. In contrast, COX-2 is inducible and is up regulated during inflammation.
Smooth muscle cells in blood vessels produce prostaglandins (PGs). PGE2 acts as a vasodilator by stimulating the Gs-protein pathway, whereas PGF2α commonly produces vasoconstriction by stimulating the Gq-protein pathway.
Vascular endothelium produces PGI2 as its primary derivative of arachidonic acid. This prostanoid is a potent vasodilator and inhibitor of platelet adhesion to the endothelium and acts through the Gs-protein pathway. Therefore, it is anti-thrombotic. These actions, although acting through different cellular mechanisms, are like those of endothelium-derived nitric oxide. Endothelial dysfunction or damage, which occurs in atherosclerosis, for example, can cause vasospasm and thrombosis.
Platelets produce TXA2, which is a potent vasoconstrictor acting through the Gq-protein pathway. Its production is enhanced during inflammation and tissue injury, and following platelet activation. TXA2 promotes vascular contraction when a vessel is cut and bleeding (hemostatic function).
Leukocytes produce leukotrienes, such as LTC4, in response to inflammation and tissue injury. Like TXA2, it is a potent vasoconstrictor that acts through the Gq-protein pathway. Leukotrienes (and prostaglandins) can also make the vascular endothelium “leakier” and therefore promote edema formation during inflammation.
Revised 11/03/2023