
 Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021)
Cardiovascular Physiology Concepts, 3rd edition textbook, Published by Wolters Kluwer (2021) Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)
Normal and Abnormal Blood Pressure, published by Richard E. Klabunde (2013)Sinoatrial Node Action Potentials
General characteristics
Cells within the sinoatrial (SA) node are the primary pacemaker site within the heart. These cells are characterized as having no true resting potential, but instead generate regular, spontaneous action potentials. Unlike non-pacemaker action potentials in the heart, the depolarizing current is carried into the cell primarily by relatively slow Ca++ currents instead of by fast Na+ currents. There are, in fact, no fast Na+ channels and currents operating in SA nodal cells. This results in slower action potentials in terms of how rapidly they depolarize. Therefore, these pacemaker action potentials are sometimes referred to as "slow response" action potentials.
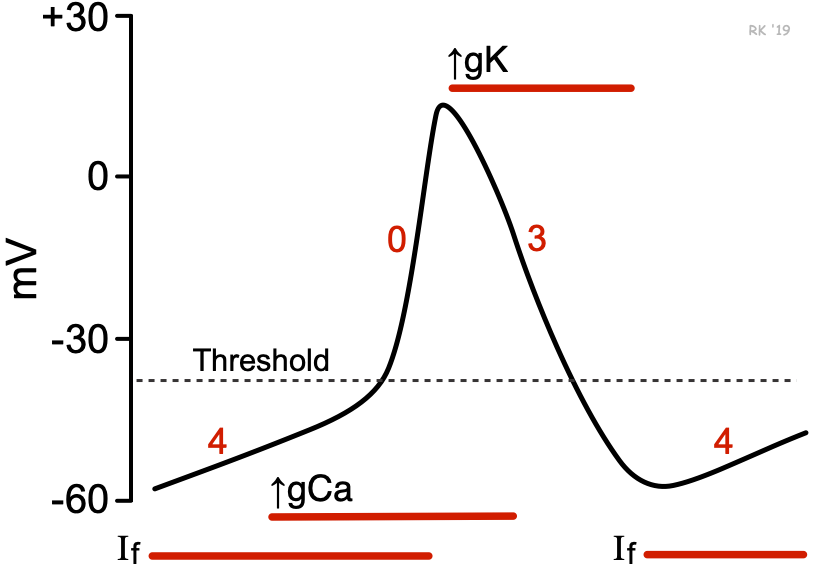 SA nodal action potentials are divided into three phases. Phase 4 is the spontaneous depolarization (pacemaker potential) that triggers the action potential once the membrane potential reaches a threshold between -40 and -30 mV). Phase 0 is the depolarization phase of the action potential. This is followed by phase 3 repolarization. Once the cell is completely repolarized at about -60 mV, the cycle is spontaneously repeated.
SA nodal action potentials are divided into three phases. Phase 4 is the spontaneous depolarization (pacemaker potential) that triggers the action potential once the membrane potential reaches a threshold between -40 and -30 mV). Phase 0 is the depolarization phase of the action potential. This is followed by phase 3 repolarization. Once the cell is completely repolarized at about -60 mV, the cycle is spontaneously repeated.
Ion channels
The changes in membrane potential during the different phases are brought about by changes principally in the movement of Ca++ and K+ across the membrane through ion channels that open and close at different times during the action potential. When a channel is opened, there is increased electrical conductance (g) of specific ions through that ion channel. Closure of ion channels causes ion conductance to decrease. As ions flow through open channels, they generate electrical currents that change the membrane potential.
At the end of repolarization, when the membrane potential is very negative (about -60 mV), ion channels open that conduct slow, inward (depolarizing) Na+ currents. These currents are called "funny" currents and abbreviated as "If". These depolarizing currents cause the membrane potential to begin to spontaneously depolarize, initiating Phase 4. As the membrane potential reaches about -50 mV, a transient or T-type Ca++ channel opens, which increases calcium conductance (gCa). As Ca++ enters the cell through these channels down its electrochemical gradient, the inward directed Ca++ currents further depolarize the cell. When the membrane depolarizes to about -40 mV, a second type of Ca++ channel opens, which further increases gCa. These are the long-lasting, or L-type Ca++ channels. Opening of these channels causes more Ca++ to enter the cell and to further depolarize the cell until an action potential threshold is reached (usually between -40 and -30 mV). It should be noted that a hyperpolarized state is necessary for pacemaker channels to become activated. Without the membrane voltage becoming very negative at the end of phase 3, pacemaker channels remain inactivated, which suppresses pacemaker currents and decreases the slope of phase 4. This is one reason cellular hypoxia, which depolarizes the cell and alters phase 3 hyperpolarization, leads to a reduction in pacemaker rate (i.e., produces bradycardia). During Phase 4 there is also a slow decline in the outward movement of K+ as the K+ channels responsible for Phase 3 continue to close. This fall in K+ conductance (gK) contributes to the depolarizing pacemaker potential.
Phase 0 depolarization is primarily caused by increased gCa through the L-type Ca++ channels that opened toward the end of Phase 4. The "funny" currents, and Ca++ currents through the T-type Ca++ channels, decline during this phase as their respective channels close. Because the movement of Ca++ through these channels into the cell is not rapid, the rate of depolarization (slope of Phase 0) is much slower than found in other cardiac cells (e.g., Purkinje cells). Those cells depend on fast sodium currents for Phase 0.
Phase 3 repolarization occurs as K+ channels open (increased gK), which increases outward directed, hyperpolarizing K+ currents. Concurrently, L-type Ca++ channels become inactivated and close, which decreases gCa and the inward depolarizing Ca++ currents.
Equilibrium potentials
During depolarization, the membrane potential (Em) moves toward the equilibrium potential for Ca++, which is about +134 mV. During repolarization, g’Ca (relative Ca++ conductance) decreases and g’K (relative K+ conductance) increases, which brings the Em closer toward the equilibrium potential for K+ (which is about -96 mV). Therefore, the action potential in SA nodal cells primarily depends on changes in Ca++ and K+ conductances, as summarized below:
Em = g'K+ (-96 mV) + g'Ca++ (+134 mV)
Although pacemaker activity is spontaneously generated by SA nodal cells, the rate of this activity can be modified significantly by external factors, such as by autonomic nerves, hormones, drugs, ions, and ischemia/hypoxia.
It is important to note that action potentials described for SA nodal cells are very similar to those found in the atrioventrcular (AV) node. Therefore, action potentials in the AV node, like the SA node, are determined primarily by changes in slow inward Ca++ and K+ currents, and do not involve fast Na+ currents. AV nodal action potentials also have intrinsic pacemaker activity, produced by the same ion currents as described above for SA nodal cells.
Revised 10/27/2023